
June’s journal club was lead by Will Beeninga (Undergrad in Katie Henzler-Wildman’s Lab). Journal club review was written by Amanda Hurley (Postdoc in Jo Handelsman’s Lab).
In August, CaSP is focusing on policy surrounding the opioid crisis. The July journal club addressed this issue by exploring the ominously-titled article in the Washington Post, “The Drug Industry’s Triumph over the DEA,” which I’ll summarize here.
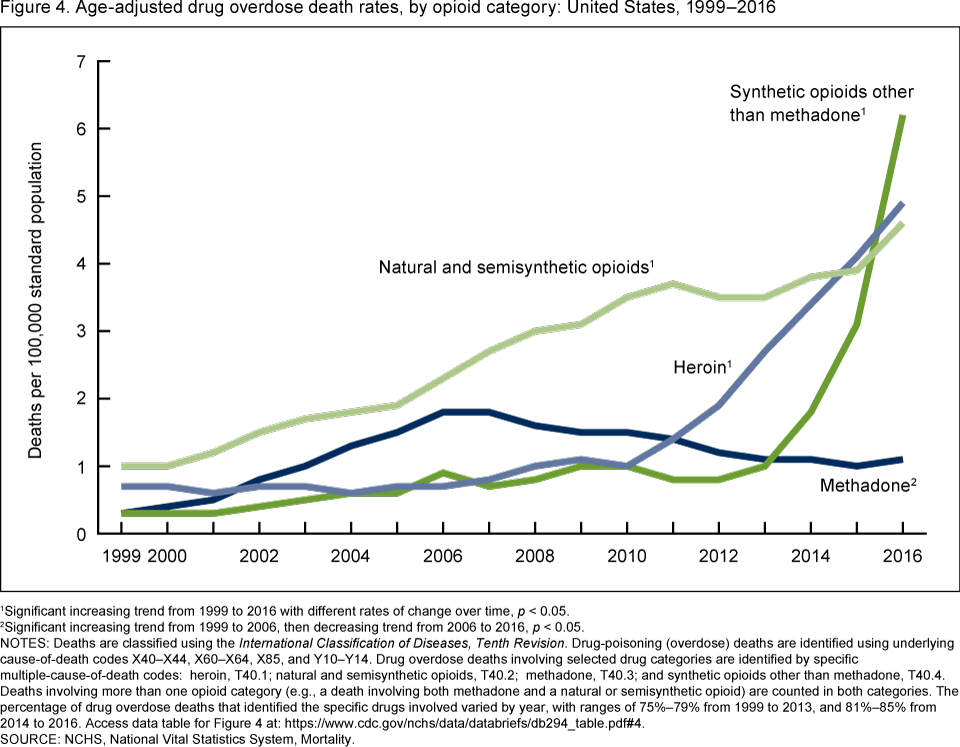
According to the CDC, the opioid epidemic arrived in three waves.The first wave started in 1999 with the steady increase of synthetic/semisynthetic opioids. The second wave in 2010 launched the steady increase in heroin deaths. And finally, in 2013, the astronomical increase in synthetic opioid deaths began. The first wave is accredited to a more aggressive attempt to manage chronic pain. In 1996, Purdue Pharma brought OxyContin to the market. In one year, from 1995 to 1996, the number of painkiller prescriptions jumped by 8 million (increasing as much as 400% from the early ‘90s). The main message from pharmaceutical companies, case studies from doctors, and pain advocates was that short-term opioid use was rarely addictive. As we know now, this is wildly untrue. As their prescriptions ended, patients turned to a more-accessible, cheaper drug of choice: heroin. The final wave of opioid deaths can be attributed to fentanyl, a synthetic opioid used for cancer pain that is 50 to 100 times more potent than heroin and, therefore, easy to overdose on. With no indication of slowing down, the opioid crisis lead the Health and Human Services secretary to declare a nationwide public health emergency in late 2017.
{kind=link}
Wednesday’s journal club focused on the policies of the Drug Enforcement Administration (DEA) targeting the “drug dealers in lab coats,” drug distributors. The main enforcement tool,based on the Controlled Substances Act of 1970, required drug companies to report suspicious orders. If the DEA noticed a suspicious order that was not reported, they asked the company to prove the legitimacy of the order in 30 days or face consequences such as fines or suspension. In the mid-2000s, drug companies shipped huge volumes of opioids to small towns and the DEA warned these companies that they were causing, according to the language of the bill, “imminent danger” to the community. For example, the distributor Miami-Luken sent about 11 million pills to a single county in West Virginia, where the population was only 25,000. The DEA eventually brought 17 cases against drug companies and manufacturers settling for over 400 million dollars.
Unfortunately, things begin to shift after 2011. The immediate suspension orders from the DEA dropped from 65 in 2011 to 8 in 2016. There are two apparent and intertwined causes. First, top DEA lawyers left the government for jobs in the pharmaceutical industry, bringing with them intimate knowledge of DEA procedurals. The former DEA lawyers torpedoed the “imminent danger” phrase of the 1970 substances act in the courtroom. Second, new legislation, partially written by Linden Barber – the DEA-turned-industry lawyer, officially restricted the definition of “imminent danger.” The legislation was co-sponsored by 23 lawmakers who received a combined $1.5 million dollars from drug lobbyists. Top DEA officials and bill sponsors were praised on the Hill for their cooperation and communication with “supply chain stakeholders.”
We wondered which was true. Should the new DEA officials be chastised for succumbing to industry pressure? Or could cooperation be the key to a mutually beneficial relationship? We then discussed alternative avenues that governments could take to stem the flow of opioids. Perhaps the “imminent danger” sentiment could be expanded on. Maybe by making drug distributors responsible for local drug overdoses, it would spark an interest in controlling the opioid epidemic. For example, should the main opioid supplier to a certain county have to pay a fine every time someone dies from drug overdose? Or maybe we could we target the demand, instead of the supply? Could fixing addiction (properly) be made profitable? The current opioid epidemic has a relatively clear beginning with no end in sight. Only by holistically addressing all facets of addiction will this country be able to gain control of the dangerous acceleration of drug use.